Aging, Connectedness and COVID: An Excerpt from ‘Together Apart’
In order to reduce the spread of the virus and to protect vulnerable persons, it is strongly advised to reduce physical contact, not to visit older persons, not to go to care homes and nursing homes.(European Federation of Psychologists’ Associations [EFPA], 2020)
This statement by EFPA is one of many recommendations that emerged in March 2020 as the health consequences of COVID-19 were being recognised internationally. In many countries, the restrictions imposed to limit the spread of the virus have seemed particularly severe for older people, due to concerns about their greater vulnerability and risk of serious illness and death. Let us be in no doubt — the advice to physically distance from one another has been an essential public health policy for protecting older people from COVID-19. But, as the previous chapter outlined, its unintentional consequence — of increasing social disconnection and loneliness — is a recognised health hazard that itself requires careful management. This chapter focuses on the particular challenges of isolation for older people as well as potential solutions.
Older people are at particular risk of poor health due to isolation
Perhaps counterintuitively, recent national surveys indicated that prior to COVID-19, older people were some of the least lonely in society (Haslam, Haslam, & Cruwys, 2019). At first sight, we might imagine this would be advantageous when it comes to combating the threat of social disconnection posed by the pandemic. However, things are not that simple. For social connections can only act as resources to bolster health and well-being when they are accessible and when they provide a vehicle to maintain and extend meaningful ties. Under conditions of lockdown, the primary means through which people connect are virtual and hence rely on technology, which is often less accessible to older people because it is unfamiliar or unaffordable. If this is the case, then older people stand to lose their social connection ‘advantage’. Furthermore, some countries have proposed ‘shielding’ older people by imposing lockdown measures only for these people — meaning their isolation is likely to be longer and more extreme than that of other groups.
This is all the more concerning because, if they become disconnected and more lonely, older people are more susceptible to the health risks associated with loneliness. Indeed, evidence shows that older people living with chronic loneliness visit their physician more often, are more likely to require rehospitalisation, and more often develop multiple chronic illnesses than their more connected counterparts (Gerst-Ermon & Jayawardhana, 2015). They also experience greater and more rapid decline in cognitive health, mobility, and mental health than those who do not feel lonely (Kuiper et al., 2015). These widespread effects across all domains of health have been attributed to the ways in which chronic loneliness compromises the immune system over time (Hawkley & Cacioppo, 2003) — predisposing lonely people to new illnesses as well as intensifying any pre-existing conditions.
From this substantial evidence base, we can predict that a major ‘shock’ to the social support system such as the COVID-19 pandemic is likely to have more serious consequences for the mental, physical and cognitive health of older adults. Moreover, where chronic loneliness emerges as a consequence of physical distancing restrictions, this will increase the likelihood of negative health outcomes (e.g., increased falls, more rapid cognitive decline) that limit a person’s capacity to live independently.
Gaining group ties mitigates the health costs of loneliness for older people
The obvious way to counteract these adverse health consequences is by striving to sustain, or if possible build, social connection. The science is also clear about the form that these connections should take — they must be meaningful, preferably multiple, and include social groups (Haslam, Jetten et al, 2018). This is evidenced by three studies which draw on the English Longitudinal Study of Ageing — a population survey with multiple waves of data from more than 18,000 people aged 50+ living in the community. The first showed that older adults who lost two social group memberships following retirement had a 12% risk of mortality over the next six years (Steffens et al., 2016). However, this risk fell to just 2% if people were able to maintain their group memberships, and to less than 1% if people gained groups in the post-retirement period.
The second study compared the effects of different forms of social engagement on cognitive integrity over three time points each separated by two years (Haslam, Cruwys, & Haslam, 2014). This found that group-based ties offer benefits for cognitive health, even after one-on-one social ties were accounted for. Furthermore, as Figure 6 shows, the group ties became even more important for cognitive health as people got older.
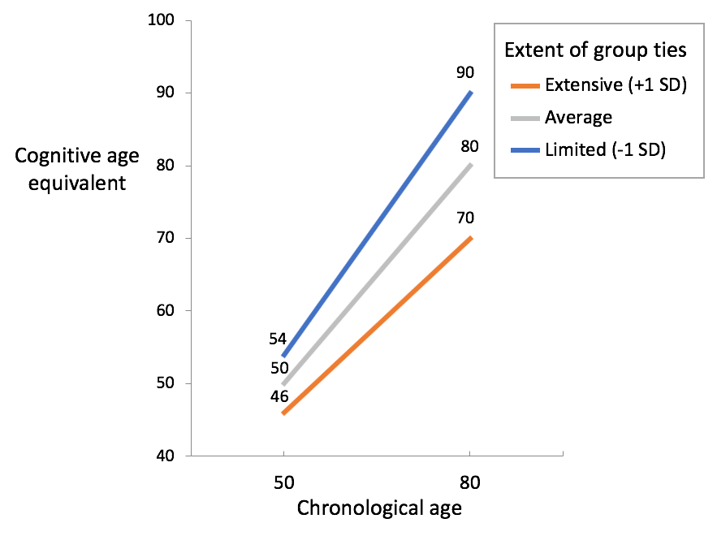
Note: This graph shows that as people get older, group ties become much more important for the preservation of their cognitive health (from Haslam, Cruwys, & Haslam, 2014).
The third study looked at the benefits of group memberships for mental health among people with a history of depression (Cruwys et al., 2013). On average, people who have experienced depression will go on to have between five and nine separate depressive episodes in their lifetime (Burcusa & Iacono, 2007), which points to the difficulty of achieving stable long-term recovery. However, Cruwys and colleagues (2013) show that joining groups can play a critical role in protecting people against relapse. In particular, they found that people with depression who joined three or more groups within two years had only a 15% risk of depression relapse six years later. This compared to a 41% risk of relapse for those who joined no groups over this period.
These population studies are backed up by evidence from experimental and intervention studies among older people living in care, which illustrate that acquiring positive group memberships (e.g., through a social club or reminiscence group) is causally linked to better mental, cognitive and physical health (Gleibs et al., 2011; Knight et al.,2010). Importantly, these effects do not arise from joining just any group. Rather, the data shows that it is only those groups that get ‘under a person’s skin’ and become internalised as an important part of their sense of self that have this power. In other words, groups are only beneficial when people identify strongly with them (Haslam, Haslam et al., 2014).
Nonetheless, like most other research in this area, this evidence of the benefits of group connectedness has been collected in contexts where people have been able to interact in close proximity. This therefore raises a key question in the COVID-19 era — can the health-related benefits of social connection still be harnessed when people are required to be physically separated from each other?
Technology can keep older people connected
More than ever, and particularly in the context of the COVID-19 pandemic, social interactions are increasingly dependent on technology. However, this shift to technology has been most prevalent in younger people. Evidencing this ‘digital divide’, prior to COVID-19 people under the age of 40 used social media platforms more than face-to-face meetings to support social interaction, whereas the opposite was true for those over 40 (Hall, 2018). With this in mind, a large number of studies have sought to investigate older people’s use of technology, with many showing that this can have benefits for well-being — not least by increasing their sense of connection to other individuals and to society more broadly.
Unsurprisingly, these efforts are more successful when older people are trained to use technology (Delello & McWhorter, 2018) or technology is adapted to make it more user-friendly (Morton et al., 2018). Even more important is investment in making virtual connection meaningful: interventions are most successful when older adults are supported to pursue their interests, such as lifelong learning, through live webcasting (Botner, 2018) and videoconferencing (Hilton et al., 2019).
However, social connection proves more challenging when people have neither the resources nor the confidence to use technology. While this can be ameliorated with resources and time, the speed with which COVID-19 restrictions were implemented allowed little time to address accessibility barriers for older people. Of course, there are other ways to connect with family and friends (e.g., through regular phone calls) and with neighbours (e.g., by interacting at a safe distance) but these often require resourcefulness, initiative, and confidence — traits often compromised by the very fact of isolation. It is for precisely this reason that working with older adults to help them retain group-based connections is so important. Finding the best way to do this is a challenge in a pandemic, but it needs to be a priority.
Explore the section of Together Apart on social (dis)connectedness
Group Threat and COVID| Katharine H. Greenaway
Risk Perception Amid COVID | Tegan Cruwys
Social Isolation Amid COVID | Sarah V. Bentley






 and the Art of Alienation")













































































